Medicare, Medicaid, and private health insurance helped fuel the opioid epidemic because they made it too easy and inexpensive for patients to get opioids, suggests a government-funded study by researchers at Johns Hopkins Bloomberg School of Public Health.
Authors of the study conclude that insurers share responsibility for the massive toll of opioid deaths because they didn’t put in precautions on the drugs to make them harder to access. They covered opioids at a low cost, didn’t discourage their prescribing, and allowed a large volume to be prescribed at once.
Recommended Stories



“Our findings suggest that both public and private insurers, at least unwittingly, have contributed importantly to the epidemic,” said Dr. G. Caleb Alexander, co-director of the Johns Hopkins Center for Drug Safety and Effectiveness and senior author of the study.
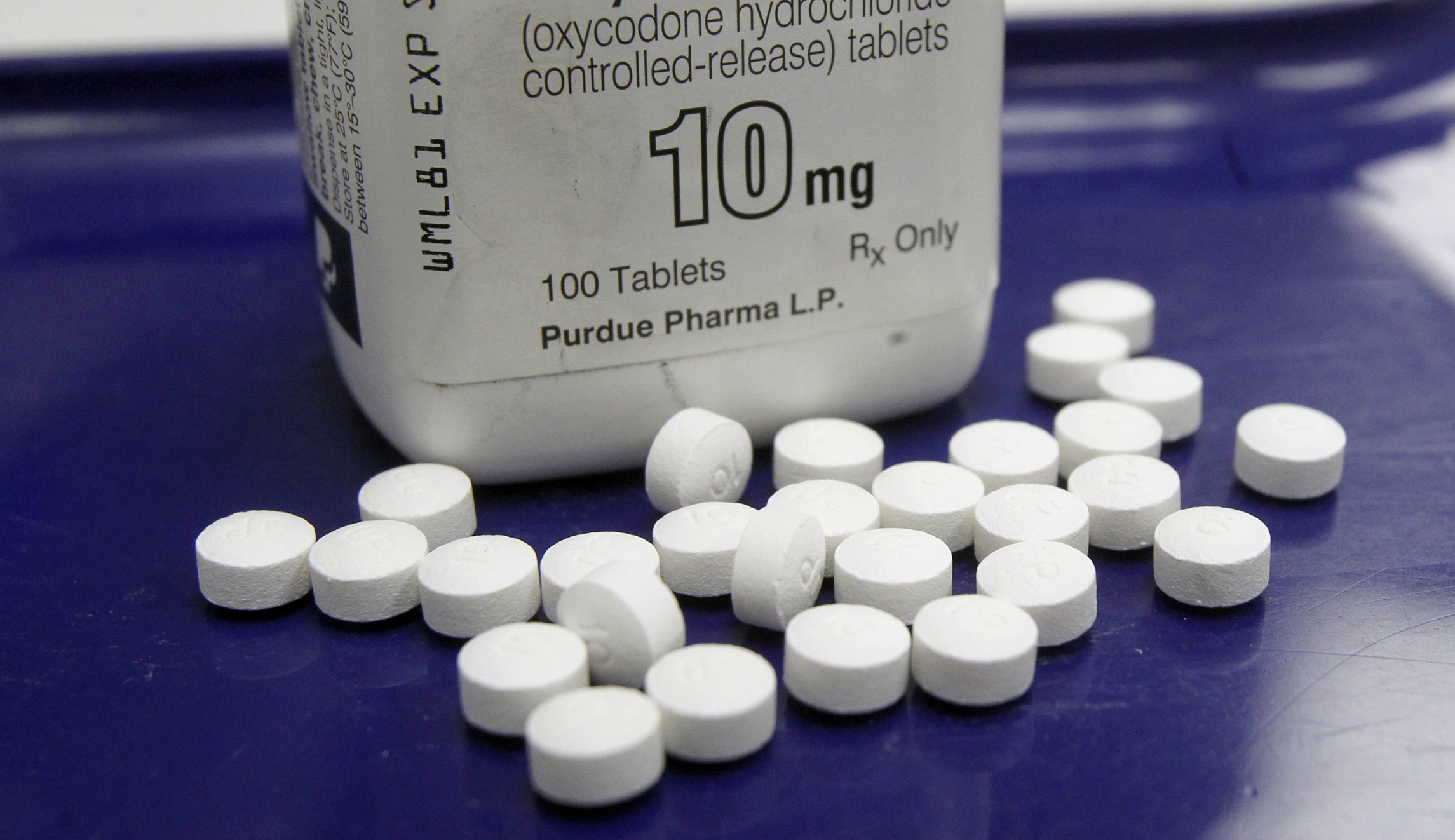
Public health experts have concluded that the overprescribing of painkillers such as Oxycontin contributed to the opioid epidemic. After patients became hooked on the drugs, they sought more easily available, cheaper, and illegal alternatives such as heroin, which can be tainted with fentanyl, an even more potent drug. The trend led to a record number of deaths in 2016, of more than 42,000 overdoses.
[Opinion: The real shame of the opioid crisis: An addiction industry that keeps preying on victims]
The dispute over whether Medicaid in particular contributed to the opioid epidemic after millions more people across the U.S. joined the program due to Obamacare has been the topic of congressional hearings and partisan attacks on Capitol Hill. The program covers pregnant women and people with disabilities and, under Obamacare, was expanded in some states to cover low-income people. Certain Republicans have argued that bringing more people into the program fueled the epidemic, though a study published in Health Affairs disputed this conclusion.
The latest study, published in the journal JAMA Network Open, suggests the overdose crisis was fueled by Medicaid as well as other coverage programs, including the Medicare program for adults 65 and older and private health insurance, which covers most people in the U.S.
Researchers analyzed 15 Medicaid plans, 15 Medicare Advantage plans, and 20 private plans in 2017, across 16 states that represent half of the U.S. population, many of which have high rates of overdoses. They also interviewed more than 43 senior healthcare executives.
They focused on 62 different medicines that doctors prescribe to treat pain in patients’ lower backs, about 30 of which were opioids and the rest were relaxants, creams, and anti-inflammatory drugs that aren’t addictive. Lower back pain is one of the most common types of pain for which opioids have been overprescribed.
The Bloomberg researchers found several practices that contributed to the overprescribing of opioids. For instance, while insurers placed limits on the number of days for which opioids could be prescribed, they often stretched those limits to 30 days, rather than a shorter amount of time, as the Centers for Disease Control and Prevention recommends. The more medicines patients have, the more likely they are to develop a dependency on the drugs.
[Also read: Doctors reduce opioid prescriptions, study finds]
Medicare, Medicaid, and private health insurers also made opioids available to patients at a cheap cost. Private plans placed 74 percent of opioids in the cheapest category, with median co-pays of only $10 for a month of pills.
Insurers failed to encourage doctors to try other nonaddictive drugs to see whether they work before prescribing opioids. A median of 9 percent of the opioids that were covered had this requirement. For private plans, the requirement was lower, at 4 percent, and in Medicare, the requirement virtually didn’t exist. Similarly, insurers for the most part didn’t set requirements for doctors to contact them about getting approval for the drug before writing a prescription, a practice that is used when drugs can have dangerous or worrisome side effects.
The authors point out that insurers have become more cautious since their study was underway.
“Insurers can either be part of the problem, or part of the solution,” Alexander said. “The good news is that an increasing number of health plans are recognizing their contribution to the epidemic and developing new policies to address it. The bad news is that we have a very long way to go.”
The study was funded by the Office of the Assistant Secretary for Planning and Evaluation, part of the Department of Health and Human Services. It used input from other federal agencies, including the National Institute on Drug Abuse of the National Institutes of Health and the Centers for Disease Control and Prevention.