For decades, Democrats and Republicans have had very different positions on drug prices. Democrats, led by Hillary Clinton portrayed drug companies—like other profitable industries—as greedy profiteers whose prices should be cut by having government ‘negotiate’ drug prices as they do in Europe, Canada and China. Indeed, Mrs. Clinton nearly wiped out the vaccine industry with her proposal to have the government purchase childhood immunizations at a government set price.
Republicans have taken a more nuanced approached. They recognized drugs have been about 12-14 percent of health care spending and that more often than not, new medicines—while expensive and risky to produce—saved lots of lives and reduced the social and economic burden of more expensive and less effective alternatives. It addressed out of pocket costs by creating a Medicare prescription drug that used market forces to keep prices down.
But that difference in approach is rapidly dissolving as out of pocket spending for medicines has soared. Many Republicans, including Donald Trump, are now embracing liberal proposals to regulate drug prices. Donald Trump has promised as President he’d negotiate with drug companies to save $400 billion a year.
But there are many problems with this proposal, not the least of which that the $400 billion a year in savings is wildly exaggerate. The United States spends $425 billion on medicines each year. The likely source of the estimate is a study from a liberal think tank’s that claimed cutting US drug costs to Denmark’s levels would save Medicare $400 billion and consumers about $112 billion over ten years.
The human cost of such negotiations is sizeable. Often it takes Denmark’s health bureaucrats three years to negotiate prices. Because the government has the power to not pay for medicines whose prices are regarded as too high, negotiations actually consist of not paying for many medicines as a tactic to extract a series of price cuts for those they cover.
Denmark, like other countries that use the same monopoly bargaining power, cut per capita drug spending by simply refusing to cover most of the newest, most effective cancer medicines. Danish cancer patients get only 30 percent of new drugs that have been developed since 2005. That’s also lowest rate in Europe (except Poland).
As a result, Denmark’s survival rates for patients with lung, colorectal and ovarian cancer are near the worst in the OECD along with United Kingdom. A recent study concluded that Denmark’s price negotiations led to underuse of potentially successful treatments. Worse, after all that Danes still pay 30 percent of the cost of drugs.
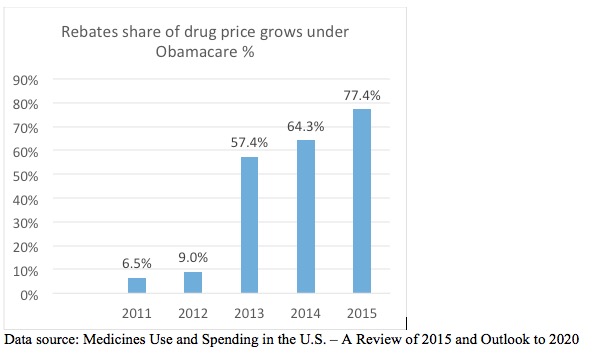
Giving Medicare power to negotiate prices would—and is—already having the same toxic effect on American consumers. Under Obamacare health plans and pharmacy benefit managers who run prescription drug programs for insurers and others have been given free reign to extract deeper savings from drug companies. Indeed drug price increases, once rebates and discounts are taken into account, have actually dropped by half since 2011. As an IMS study observes: “The average net price for brands already in the market is estimated to have increased by 2.8% in 2015, down from 5.1% in 2014 and significantly lower than seen in prior years.”
Just as in Europe, under Obamacare insurers and PBMs have simply excluded more drugs for reimbursement. Express Scripts has 66 products on its 2015 formulary exclusion list, compared with 48 in 2014. CVS Caremark͛s 2015 list has 95 products, including 72 carryovers from the 2014 edition. CVS Caremark removed a mere 34 drugs from its 2012 standard national formulary.
The discount off of retail drug prices is substantial. On average, biopharmaceutical companies provide discounts and rebates that reduce the price of medicines by about 30-40 percent, and often to prices lower than in Europe. Spending on drugs in outpatient settings,, hospital and nursing homes increased by 12 percent in 2015 to about $425 billion. Drug and biotech companies made $310 billion of that total revenue. The other $115 billion are rebates on retail prices that go to insurers, pharmacy benefit management companies such as Express Scripts that administer drug benefits, hospitals and government coffers.
Under Obamacare, the spread between price increases faced by consumers and what special interests pocket has surged. While prices net of rebates have declined, the share of overall price hikes has leaped from 6.5 percent of price increases to 80 percent.
Incredibly, consumers do not directly benefit from the $115 billion. Insurers and PBMs claim the rebates ensure patients have affordable access to medicines. In fact, the rebates only guarantee that a medicine will be on drug formularies. Rather, under Obamacare the number of health plans that restrict access to new drugs has increased. Between 30-50 percent of insurers place drugs for HIV, cancer and multiple sclerosis Agents including available generics, on the highest tier.
As a result, the number of Obamacare patients facing cost sharing of up to 40 percent has soared even as rebate revenue increased. The mounting cost, combined with European style limits on access to new drugs, make people with breast cancer, HIV, multiple sclerosis and heart disease sicker.
So why don’t rebates and discounts go to patients? In large part, rebates are a guaranteed source of cash for big insurers, PBMs and hospital systems. Obamacare institutionalize this practice by specifically discourages drug companies from using rebates for reducing cost-sharing and “encourages (insurance) issuers to reject such third party payments“.
Republicans can amend Obamacare to allow companies to cut prices and provide consumers with some of $115 billion in rebates and discounts. In doing so, Republicans could strike a blow for patients instead of pushing for Danish style price controls that enrich the government and handful of companies who profit from this Obamacare ripoff.